Water in the head hydrocephalus of the foal
Water in the head hydrocephalus of the foal
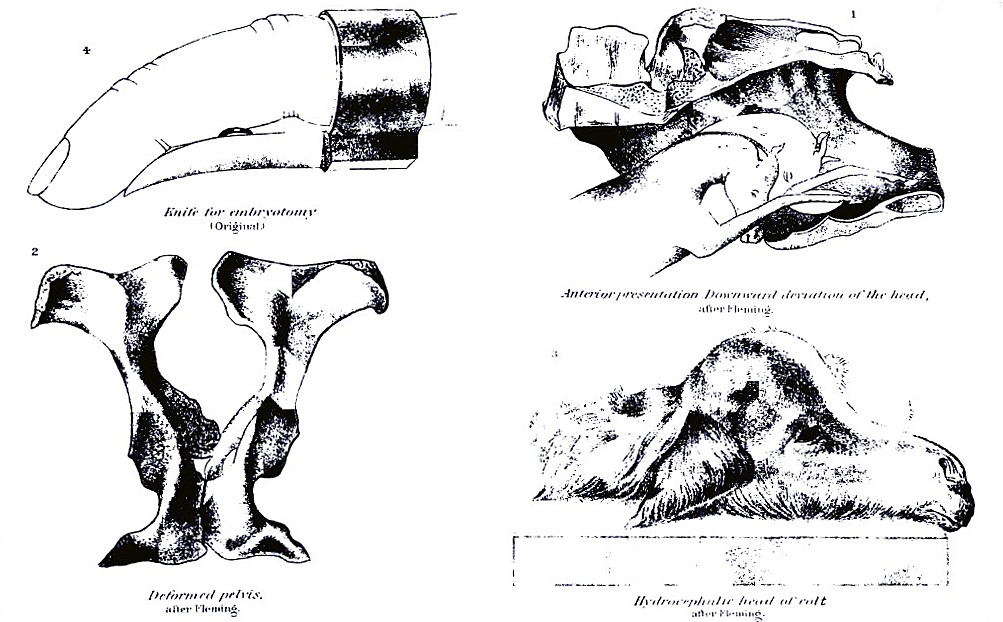
Water in the head (hydrocephalus) of the foal. This consists in the excessive accumulation of liquid in the ventricles of the brain so that the cranial cavity is enlarged and constitutes a great, projecting, rounded mass occupying the space from the eyes upward. (See Plate XIII, fig. 3.) With an anterior presentation (fore feet and nose) this presents an insuperable obstacle to progress, as the diseased cranium is too large to enter the pelvis at the same time with the fore arms. With a posterior presentation (hind feet) all goes well until the body and shoulders have passed out, when progress is suddenly arrested by the great bulk of the head. In the first case, the oiled hand introduced along the face detects the enormous size of the head, which may be diminished by puncturing it with a knife or trocar and cannula in the median line, evacuating the water and pressing in the thin, bony walls. With a posterior presentation, the same course must be followed; the hand passed along the neck will detect the cranial swelling, which may be punctured with a knife or trocar. Oftentimes with an anterior presentation the great size of the head leads to its displacement backward, and thus the fore limbs alone engage in the passages. Here the first object is to seek and bring up the missing head, and then puncture it as above suggested.

PLATE XII.
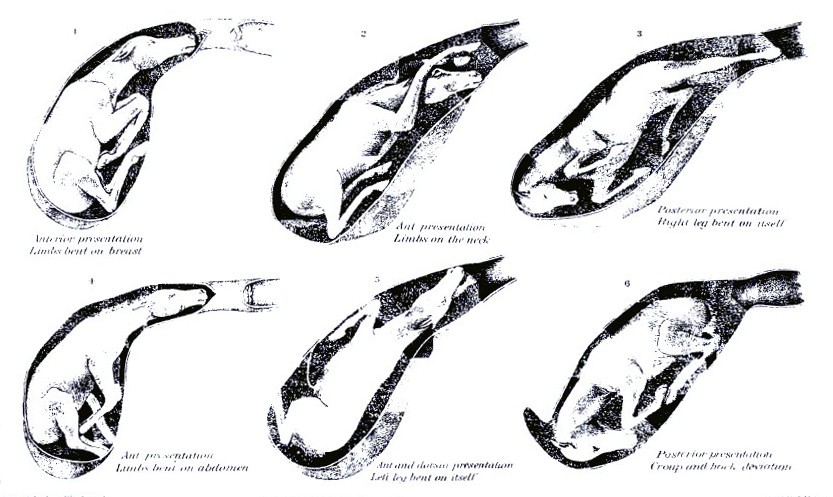
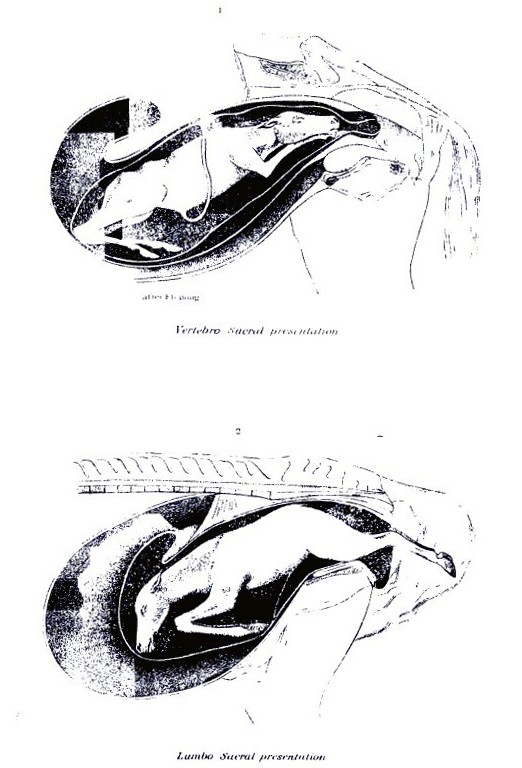
NORMAL PRESENTATIONS.

PLATE XIII.
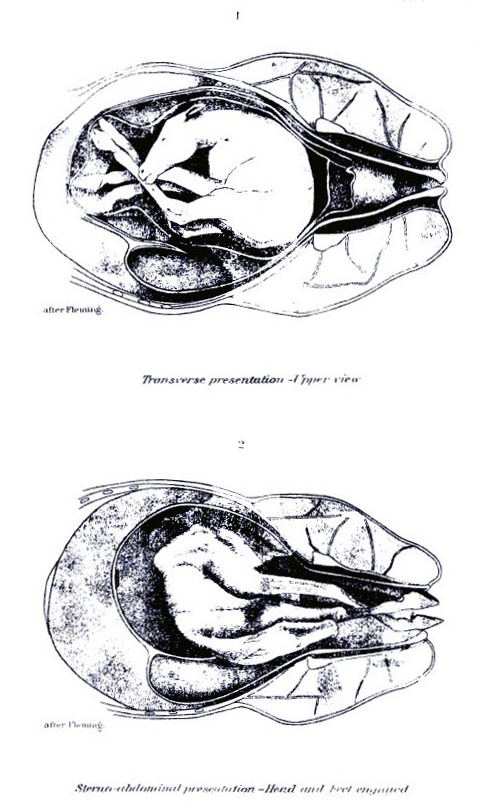
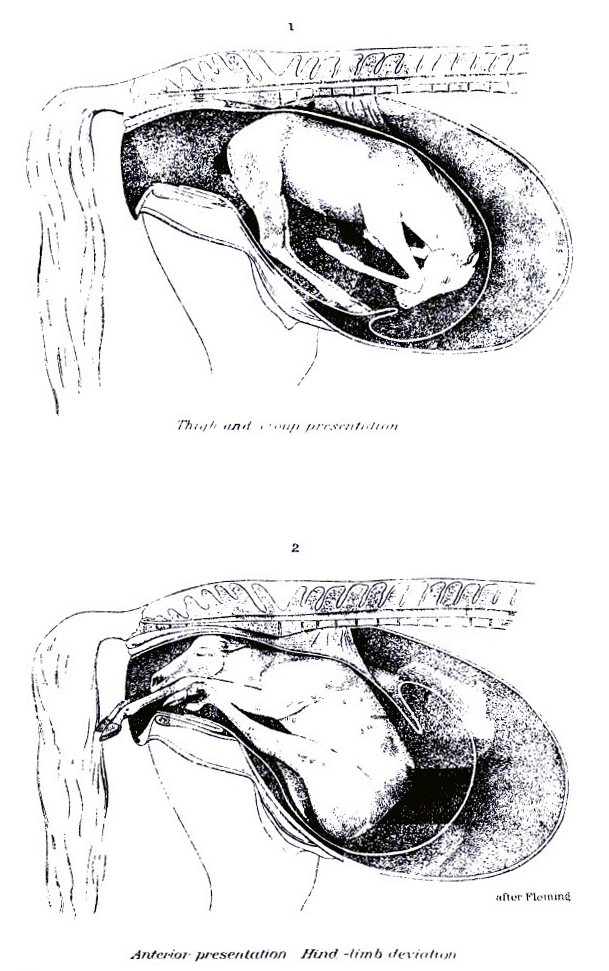
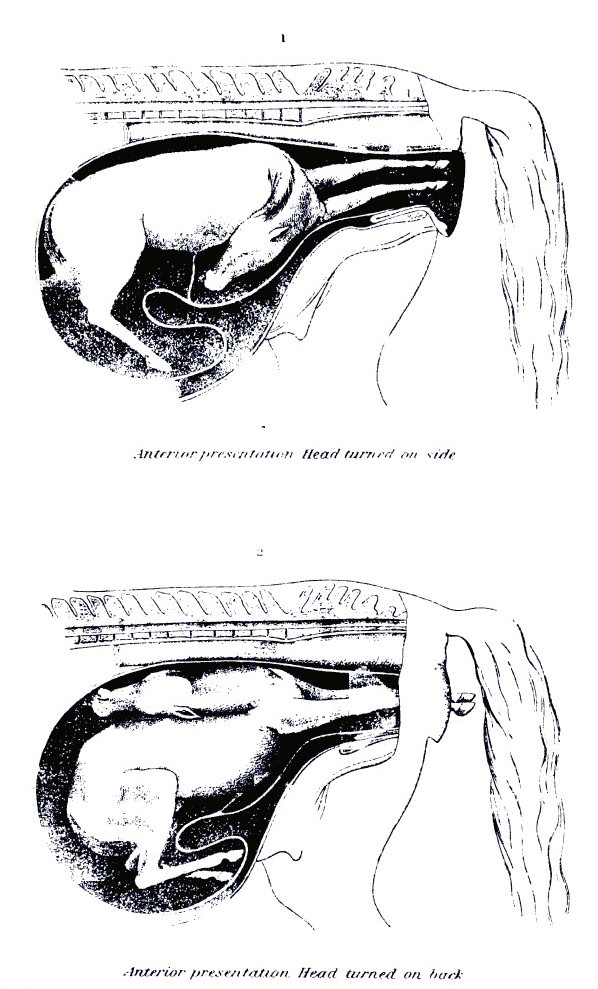
SOME FACTORS IN DIFFICULT LABOR.

PLATE XIV.
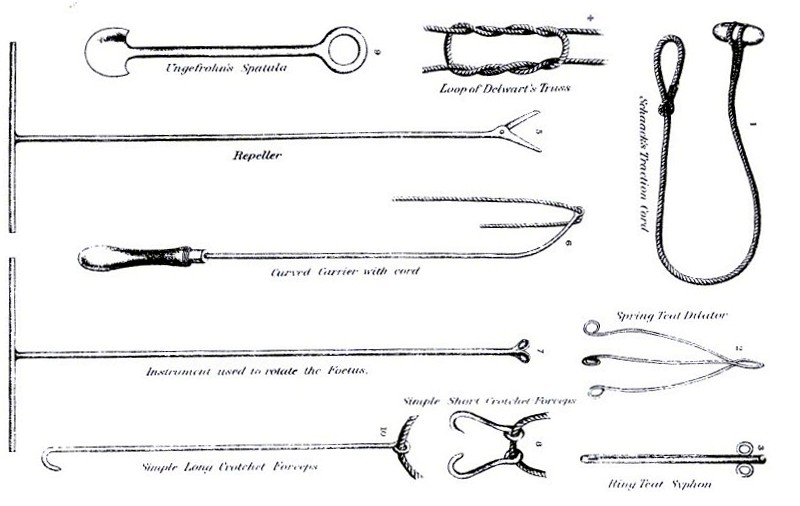
INSTRUMENTS USED IN DIFFICULT LABOR. Ascites, or dropsy of the abdomen in the foal. The accumulation of liquid in the abdominal cavity of the fetus is less frequent, but when present it may arrest parturition as completely as will hydrocephalus. With an anterior presentation the foal may pass as far as the shoulders, but behind this all efforts fail to effect a further advance. With a posterior presentation the hind legs as far as the thighs may be expelled, but at this point all progress ceases. In either case the oiled hand, passed inward by the side of the foal, will detect the enormous distension of the abdomen and its soft, fluctuating contents. The only course is to puncture the cavity and evacuate the liquid. With the anterior presentation this may be done with a long trocar and cannula, introduced through the chest and diaphragm, or with a knife an incision may be made between the first two ribs and the lungs and heart cut or torn out, when the diaphragm will be felt projecting strongly forward, and may be easily punctured. Should there not be room to introduce the hand through the chest, the oiled hand may be passed along beneath the breast bone and the abdomen punctured. With a posterior presentation the abdomen must be punctured in the same way, the hand, armed with a knife protected in its palm, being passed along the side of the flank or between the hind limbs. It should be added that moderate dropsy of the abdomen is not incompatible with natural delivery, the liquid being at first crowded back into the portion of the belly still engaged in the womb, and passing slowly from that into the advanced portion as soon as that has cleared the narrow passage of the pelvis and passed out where it can expand.
General dropsy of the fetus. In this case the tissues generally are distended with liquid, and the skin is found at all points tense and rounded, and pitting on pressure with the fingers. In some such cases delivery may be effected after the skin has been punctured at narrow intervals to allow the escape of the fluid and then liberally smeared with fresh lard. More commonly, however, it can not be reached at all points to be so punctured nor sufficiently reduced to be extracted whole, and resort must be had to embryotomy.
Emphysema, or swelling of the fetus with gas. This has been described as occurring in a living fetus, but I have met with it only in the dead and decomposing foal after futile efforts had been made for several days to effect delivery. These cases are very difficult, as the foal is inflated to such extent that it is impossible to advance it into the passages, and the skin of the fetus and the walls of the womb and vagina have become so dry that it is impracticable to cause the one to glide on the other. The hair comes off any part that may be seized, and the case is rendered the more offensive and dangerous by the very fetid liquids and gases. The only resort is embryotomy, by which I have succeeded in saving a valuable mare that had carried a colt in this condition for four days.
Contractions of muscles. The foal is not always developed symmetrically, but certain groups of muscles are liable to remain short, or to shorten because of persistent spasmodic contraction, so that even the bones become distorted and twisted. This is most common in the neck. The bones of this part and even of the face are drawn to one side and shortened, the head being held firmly to the flank and the jaws being twisted to the right or left. In other cases the flexor muscles of the fore limbs are contracted so that the latter are strongly bent at the knee. In neither of these cases can the distorted part be extended and straightened, so that body or limbs must necessarily present double, and natural delivery is rendered impossible. The bent neck may sometimes be straightened after the muscles have been cut on the side to which it is turned, and the bent limbs after the tendons on the back of the shank bone have been cut across. Failing to accomplish this, the next resort is embryotomy.
Inclosed ovum, or tumors of the fetus. Tumors or diseased growths may form on any part of the foal, internal or external, and by their size impede or hinder parturition. In some cases what appears as a tumor is an imprisoned and undeveloped ovum which has grafted itself on the fetus. These are usually sacculated, and may contain skin, hair, muscle, bone, and other natural tissues. The only course to be pursued in such cases is to excise the tumor, or, if this is not feasible, to perform embryotomy.
Monstrosities. Monstrosity in the foal is an occasional cause of difficult parturition, especially such monsters as show excessive development of some part of the body, a displacement or distortion of parts, or a redundancy of parts, as in double monsters. Monsters may be divided into
(1) Monsters with absence of parts absence of head, limb, or other organ.
(2) Monsters with some part abnormally small dwarfed head, limb, trunk, etc.
(3) Monsters through unnatural division of parts cleft head, trunk, limbs, etc.
(4) Monsters through absence of natural divisions absence of mouth, nose, eyes, anus, confluent digits, etc.
(5) Monsters through fusion of parts one central eye, one nasal opening, etc.
(6) Monsters through abnormal position or form of parts curved spine, face, limb, etc.
(7) Monsters through excess of formation enormous head, supernumerary digits, etc.
(8) Monsters through imperfect differentiation of sexual organs hermaphrodites.
(9) Double monsters double-headed, double-bodied, extra limbs, etc.
Causes. The causes of monstrosities appear to be very varied. Some monstrosities, like extra digits, absence of horns or tail, etc., run in families and are produced almost as certainly as color or form. Others are associated with too close breeding, the powers of symmetrical development being interfered with, just as in other cases a sexual incompatibility is developed, near relatives failing to breed with each other. Mere arrest of development of a part may arise from accidental disease of the embryo; hence vital organs are left out, or portions of organs, like the dividing walls of the heart, are omitted. Sometimes an older fetus is inclosed in the body of another, each having started independently from a separate ovum, but the one having become embedded in the semifluid mass of the other and having developed there simultaneously with it, but not so largely nor perfectly. In many cases of redundance of parts the extra part or member has manifestly developed from the same ovum and nutrient center with the normal member to which it remains adherent, just as a new tail will grow out in a newt when the former has been cut off. In the early embryo, with its great powers of development, this factor can operate to far greater purpose than in the adult animal. Its influence is seen in the fact pointed out by St. Hilaire that such redundant parts are nearly always connected with the corresponding portions in the normal fetus. Thus superfluous legs or digits are attached to the normal ones, double heads or tails are connected to a common neck or rump, and double bodies are attached to each other by corresponding points, navel to navel, breast to breast, back to back. All this suggests the development of extra parts from the same primary layer of the impregnated and developing ovum. The effect of disturbing conditions in giving such wrong directions to the developmental forces is well shown in the experiments of St. Hilaire and Valentine in varnishing, shaking, and otherwise breaking up the natural connections in eggs, and thereby determining the formation of monstrosities at will. So, in the mammal, blows and other injuries that detach the fetal membranes from the walls of the womb or that modify their circulation by inducing inflammation are at times followed by the development of a monster. The excitement, mental and physical, attendant on fright occasionally acts in a similar way, acting probably through the same channels.
The monstrous forms liable to interfere with parturition are such as, from contracted or twisted limbs or spine, must be presented double; where supernumerary limbs, head, or body must approach the passages with the natural ones; where a head or other member has attained to an unnatural size; where the body of one fetus has become inclosed in or attached to another, etc.
Extraction is sometimes possible by straightening the members and obtaining such a presentation as will reduce the presenting mass to its smallest and most wedgelike dimensions. To effect this it may be needful to cut the flexor tendons of bent limbs or the muscles on the side of a twisted neck or body; one or more of the manipulations necessary to secure and bring up a missing member may be required. In most cases of monstrosity by excess, however, it is needful to remove the superfluous parts, in which case the general principles employed for embryotomy must be followed. The Caesarean section, by which the fetus is extracted through an incision in the walls of the abdomen and womb, is inadmissible, as it practically entails the sacrifice of the mare, which should never be done for the sake of a monster. (See "Embryotomy," p. 202.)
Entrance of twins into the passage at once. Twins are rare in the mare, and still more rare is the impaction of both at once into the pelvis. The condition would be easily recognized by the fact that two fore limbs and two hind would occupy the passage at once, the front of the hoofs of the fore feet being turned upward and those of the hind feet downward. If both belonged to one foal, they would be turned in the same direction. Once recognized, the condition is easily remedied by passing a rope with a running noose round each foot of the foal that is furthest advanced or that promises to be most easily extracted, and to push the members of the other fetus back into the depth of the womb. As soon as the one fetus is fully engaged into the passage it will hold its place and its delivery will proceed in the natural way.